













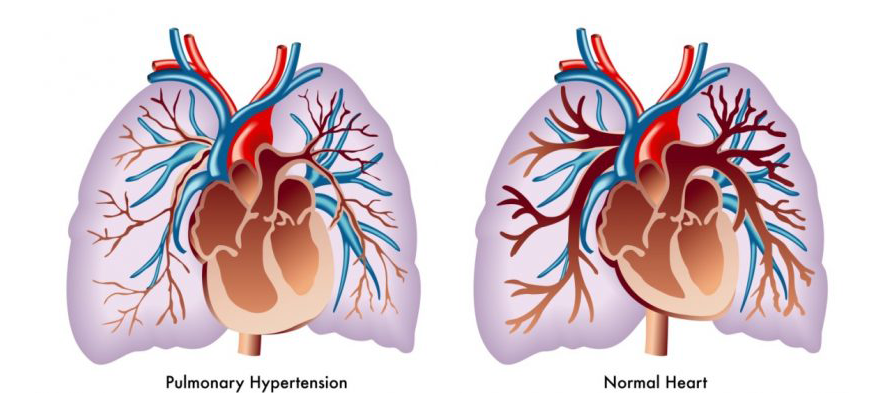
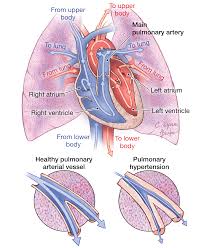
Pulmonary hypertension (PH) is a grave and rare lung disease that directly affects the pulmonary arteries, leading to elevated blood pressure. The disease causes the thickening and narrowing of the arteries that pump blood into the heart’s right ventricle. Thus, the heart of a person with PH tends to be highly stressed, which could lead to conditions such as weakened and enlarged heart, angina, and eventually heart failure.
Sleep apnoea could be considered as a potentially critical sleep disease that causes a patient to repeatedly stop breathing for short periods during sleep. Sleep apnoea is one of the most common triggers for the development of pulmonary hypertension.
Sleep Apnoea and Pulmonary Hypertension
Sleep apnoea comorbidities include diabetes, hypertension, ischemic heart disease, vascular disease, stroke, arrythmias and congestive heart failure. Thus, sleep apnoea is also a common denominator for the development not of only pulmonary hypertension but also cardiovascular disease. Research indicates that hypercapnia (elevated carbon dioxide in the body) repetitive nighttime arterial oxygen desaturation (low blood oxygen concentration) are the two main factors that contribute to the increase in pulmonary artery pressure.
An adult needs at least a full 8-hour of uninterrupted sleep for his body to repair and mend damage to the cellular level. Even the human growth hormone (HGH) is only release during deep sleep, which is achievable only during long periods of consolidated sleep.
Constant lack of sleep, or poor sleep greatly diminishes the body’s ability to recharge and repair. Obesity and aging are common risk factors for developing PH. Aging cannot be controlled while obesity can be effectively controlled and managed. If obstructive sleep apnoea (OSA) or any related sleep-disordered breathing condition, remains undiagnosed and untreated, the development and eventual progression of PH is a certainty.
Treatment of OSA and PH
According to researchers from the American College of Chest Physicians, between 17 and 53 percent of people with sleep apnea also develop pulmonary hypertension. The repeated loss of oxygen in the bloodstream due to OSA and other variants of sleep apnoea increases the pressure of the pulmonary artery.
Any 10-second, or longer, cessation in breathing during sleep is considered an apnoea. The frequency and length of apneas determine the amount of loss of oxygen in the blood. Any significant loss of blood oxygen will increase the carbon dioxide level in the blood. The decrease and increase of oxygen and carbon dioxide in the blood will stress the cardiopulmonary system, which could lead to other complications such as pulmonary hypertension. The cessation of breathing during sleep also causes negative changes to internal lung pressure, which could affect the heart.
A person diagnosed with PH can opt to have a sleep study to determine if his PH is linked to undiagnosed or untreated obstructive sleep apnoea.
Treatment for OSA- related PH is through the use of continuous positive airway pressure (CPAP). Studies have indicated that CPAP therapy can efficiently reduce pressure in the pulmonary artery.
Obesity is a controllable risk factor of both OSA and PH. An obese person with both OSA and PH must reduce his weight.
If you or any of your family has OSA or sleep apnoea-related PH, call us now.
1300 750 006
















