













Obstructive sleep apnoea or OSA is a sleep disorder involving either cessation of breath or a marked decreased in airflow when one is breathing. OSA is the most common type of sleep disorder relating to breathing, and is highly characterised by episodes of upper airway collapse while one is sleeping. Each episode is associated with repeated arousals from sleep and oxyhemoglobin desaturations. OSA that is linked to excessive daytime sleepiness is referred to as obstructive sleep apnoea syndrome or obstructive sleep apnoea-hypopnoea syndrome.
Signs and Symptoms of OSA
Symptoms of OSA are subtle. The condition could be present for years before a person realises he needs to seek medical help.
Night time symptoms may include unusually loud, habitual snoring that is bothersome to others. Cessation of breath (apnoeas) happens and is often interrupted with snoring that ends with a snort. Most experience gasping and choking that arouse them from sleep. Others exhibit nocturia, wherein there is a need to wake up several times at night to pass urine. Most patients experience insomnia or restless sleep; tossing and turning during the night; frequent arousals from sleep.
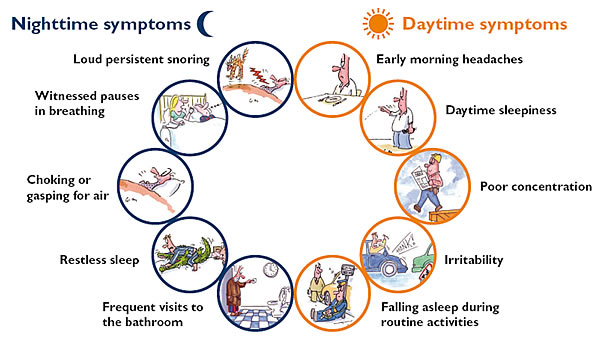 Morning headache and dry or sore throat are common symptoms. A person with undiagnosed OSA may experience excessive daytime sleepiness while doing quiet activities such as watching TV or reading. In cases of severe OSA, a patient may feel sleepy even when working or driving. Daytime fatigue is common. His concentration and short-term memory are negatively affected. Depression, anxiety, personality and mood changes may happen. Decrease in libido and impotence are also possible signs. Hypertension and gastroesophageal reflux are also symptoms of obstructive sleep apnoea.
Morning headache and dry or sore throat are common symptoms. A person with undiagnosed OSA may experience excessive daytime sleepiness while doing quiet activities such as watching TV or reading. In cases of severe OSA, a patient may feel sleepy even when working or driving. Daytime fatigue is common. His concentration and short-term memory are negatively affected. Depression, anxiety, personality and mood changes may happen. Decrease in libido and impotence are also possible signs. Hypertension and gastroesophageal reflux are also symptoms of obstructive sleep apnoea.
Diagnosis of OSA
People with OSA generally have a body mass index that is greater than 30kg/m2. The neck circumference in men is usually greater than 17 inches or 43 cm, and in women, greater than 15 inches or 37 cm. Though the general physical examination is normal, hypertension is common to patients with OSA.
An evaluation of a patient suspected with OSA may include findings such as:
• increased or abnormal Mallampati score which is an indication for difficult tracheal intubation
• indication of the narrowing of the lateral airways walls (for men only)
• enlarged tonsils (3+ to 4+)
• retrognathia or abnormal posterior positioning of the mandible
• or micrognathia which having a lower jaw that is smaller than normal
• large degree of teeth protrusion (overjet)
• high arched hard palate
• systemic arterial hypertension and pulmonary hypertension
• congestive heart failure
• stroke
• type 2 diabetes
• metabolic syndrome
Generally, polysomnography or an overnight sleep study is needed to diagnose OSA. Routine laboratory tests and pulmonary function tests are not helpful in diagnosing OSA. A thyrotropin test on a patient with suspected OSA and hypothyroidism is helpful.
Find a clinic or call us now for a consultation 1300 750 006.
















