Cognitive performance is also affected. There are studies that indicate that sleep apnoea leads to slow thinking, lower intelligence quotient, poor creativeness, and brain fog.
What is brain fog?

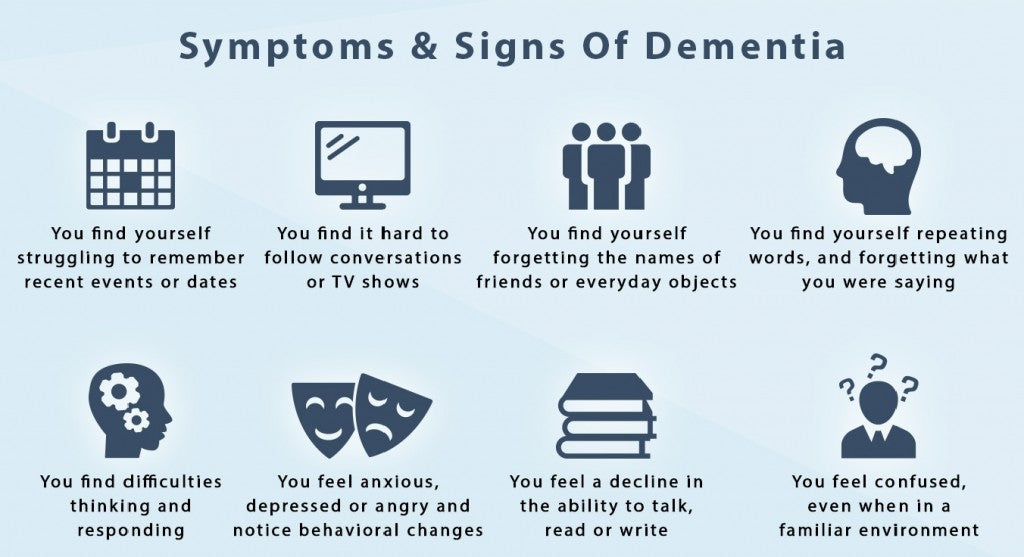
Brain fog or brain fatigue is a mental state wherein the person suffering from it exhibits poor memory recall, lack of focus and marked reduced mental acuity. This mental confusion can manifest without much warning, and the episodes can be mild to severe. If the cause of brain fog is not quickly and accurately diagnosed and treated, the episodes may reach a point wherein the person’s personal and professional life is affected.
Symptoms
Brain fog is medically termed cognitive dysfunction. A person suffering from brain fog will have difficult remembering why he came into any room. He might have to read and re-read a paragraph because he cannot remember what he read. He might be so absorbed on his daily task and not interact socially. He might feel great physically but not mentally. Remembering particular things, words, and processes could be quite a struggle, and routine tasks might require extra effort to do.
Common Causes of Brain Fog
Lack of Sleep
There are various factors that may cause brain fatigue and lack of sleep is one of them. The human body needs sleep to recover from its daily tasks. The brain needs rest and sleep too in order to recuperate from the tens of thousands of processes it does during one’s waking hours. When sleep is interrupted on occasions due to sickness or late work or studies, the sleep interruption is temporary and will not likely lead to brain fog. However, if a person’s nighttime sleep is interrupted on a regularly or daily, he is more likely to experience brain fatigue each morning. There are those who shake off brain fog with a cup of espresso, but for those who are suffering from a form of sleep disorder such as sleep apnoea, brain fog cannot be easily shaken off.
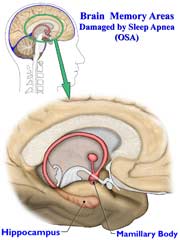
Scientific studies indicate that cognitive dysfunction may be caused by chronic sleep interruptions or difficulties across all age brackets. This means narcolepsy, insomnia, circadian rhythm disorder, restless leg disorder, shift work sleep disorder, and more, are also risk factors for brain fog. Studies also indicate that brain fatigue in patients with obstructive sleep apnoea (OSA) is quite common. This could be explained by another study suggesting that diminished oxygenation of the blood is the main culprit for memory problems and physical deficiencies.
Other Causes of Brain Fog
Stress is known to negatively affect the body, which could lead to sickness, including brain fog. An average person should be able to handle normal daily stress. If he starts to show brain fog, then the possibility of an underlying condition becomes real.
Neurological Disorders that may lead to brain fatigue include lupus, fibromyalgia, multiple sclerosis and chronic fatigue syndrome.
Diabetes causes glucose levels in the blood to fluctuate. Since glucose is the main energy source of the brain, brain fog may occur.
Menopause causes hormones to fluctuate thus women going through this phase may experience brain fatigue.
Deficiencies in nutrients and side effects of particular medications may also cause brain fatigue.
Treatment for Brain Fog
It is possible to treat brain fog. A study showed that 20 patients with severe OSA manifested brain fog. After undergoing CPAP therapy, their brain fatigue improved significantly.
If a person lacks sleep, then he should get to the root of his sleeping disorder to explore possible treatment. If the interrupted sleep is due to sleep apnoea, then consulting with a sleep doctor for correct diagnosis and treatment approach. In such case, CPAP therapy is the correct treatment.
Call us now for consultation. 1300 750 006
]]>





 The researchers of the American College of Physicians Clinical Guidelines Committee have reviewed studies pertaining to the effects of the different approaches in the treatment of obstructive sleep apnoea. According to the team of scientists, weight loss and CPAP therapy are still the best options in the treatment of obstructive sleep apnoea (Epstein, 2018).
The researchers of the American College of Physicians Clinical Guidelines Committee have reviewed studies pertaining to the effects of the different approaches in the treatment of obstructive sleep apnoea. According to the team of scientists, weight loss and CPAP therapy are still the best options in the treatment of obstructive sleep apnoea (Epstein, 2018).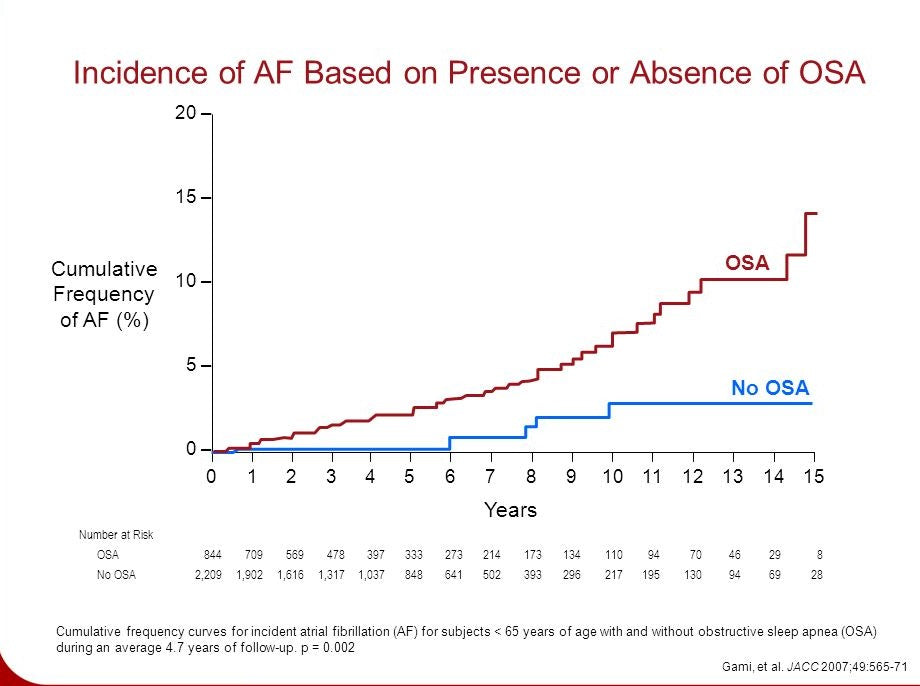
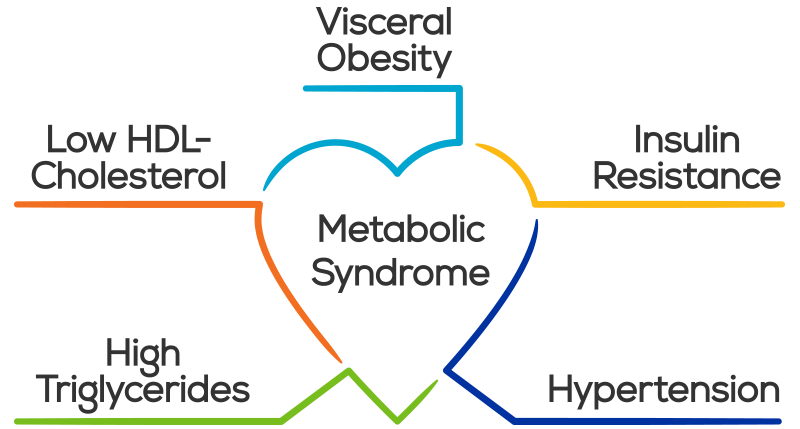

 One of the most common causes of sleep apnoea is excessive weight gain as attested by a study done by the National Center for Biotechnology Information. This study qualified that more than 50% of OSA patients are overweight and that their excess weight tends to accumulate around the neck. On the other hand, OSA itself has shown to cause weight gain too. This is due to a compromised sleep cycle that wrecks the normal rhythm of the hormones that regulate hunger.
One of the most common causes of sleep apnoea is excessive weight gain as attested by a study done by the National Center for Biotechnology Information. This study qualified that more than 50% of OSA patients are overweight and that their excess weight tends to accumulate around the neck. On the other hand, OSA itself has shown to cause weight gain too. This is due to a compromised sleep cycle that wrecks the normal rhythm of the hormones that regulate hunger. Supine sleepers are more at risk of developing sleep apnoea, but the condition could develop for prone and side sleepers as well. Supine or back sleepers have the weight of their neck and surrounding tissues and muscles forcing the airway. This causes obstruction and restrictions on the airway during sleep, which may lead to sleep apnoea. It will be more beneficial for most people to sleep on their side.
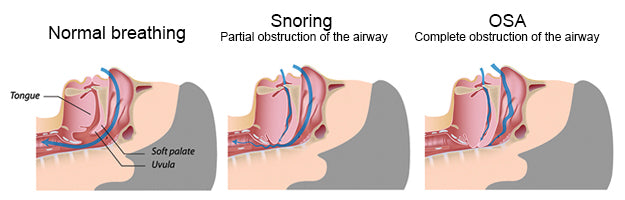
Supine sleepers are more at risk of developing sleep apnoea, but the condition could develop for prone and side sleepers as well. Supine or back sleepers have the weight of their neck and surrounding tissues and muscles forcing the airway. This causes obstruction and restrictions on the airway during sleep, which may lead to sleep apnoea. It will be more beneficial for most people to sleep on their side.